You are here




When the Nearest Hospital Is Two Hours Away: America’s Maternity Deserts
We’ve turned birth into a consumer experience. Hospital or birth center. Epidural or no epidural. Diffusers and dim lighting and the right playlist.
We talk about birth plans like everyone is working from the same menu.
But for millions of pregnant women in this country, the birth plan is much simpler: get in the car, drive as far as it takes, and hope you don’t run out of time.
What Is a Maternity Desert?
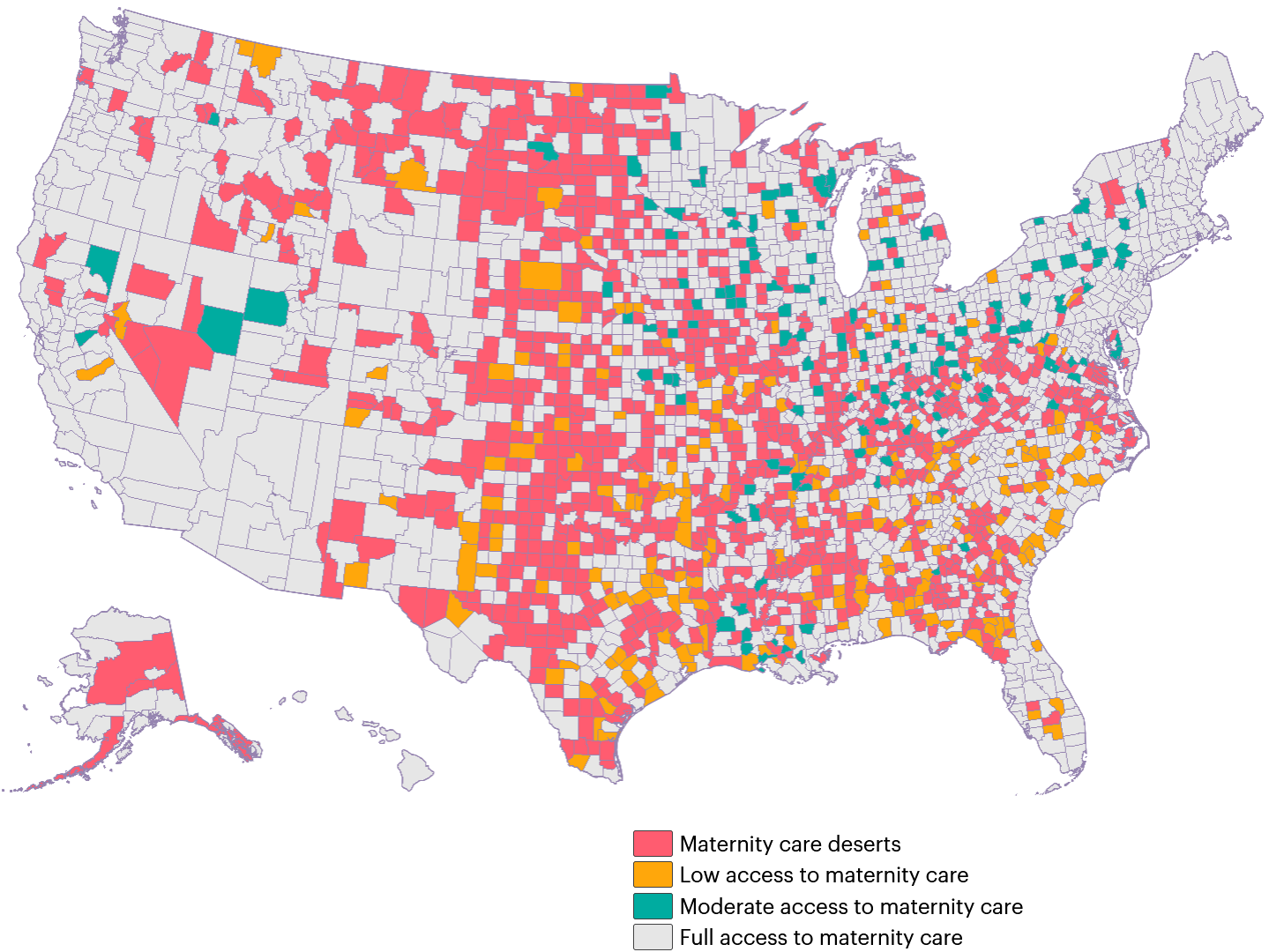
A maternity desert is a U.S. county — or a cluster of counties — with no hospital offering obstetric care and no birth center. No OB. No midwife. No labor and delivery unit. Nowhere to go when you go into labor.
The March of Dimes defines it plainly: zero obstetric providers, zero birth centers. A “low access” area is where providers technically exist but are so outnumbered they might as well not be there1. The American College of Obstetricians and Gynecologists (ACOG) warns that expectant mothers living in maternity deserts need to have a travel plan prepared in case of an obstetric emergency2.
These aren’t remote anomalies. They’re a national pattern hiding in plain sight.
Where Are the Deserts?
More than 35% of U.S. counties qualify as maternity care deserts or low-access areas1. Over 2.3 million women of childbearing age live in them. More than 1 in 12 women of reproductive age in the United States live in a maternity desert, and these areas are associated with roughly 150,000 births each year.
The problem is most concentrated in the rural South and Midwest — including states such as Mississippi, Alabama, Arkansas, and Wyoming1. The map isn’t random. It follows rural poverty, hospital closures, and the financial pressure that makes obstetric units unsustainable for small hospitals1,2.
This isn’t geography. It’s policy.
Visit this interactive map from the March of Dimes to locate the Maternity Deserts:
Who Gets Left Behind
The geography of maternity deserts overlaps almost exactly with the geography of maternal health disparities. That’s not a coincidence.
Women in these areas are more likely to be Black, Indigenous, or Latina. More likely to be on Medicaid. More likely to be young, uninsured, or without reliable transportation. More likely to be working jobs that don’t offer paid time off for prenatal appointments — even if they could somehow get to one.
And when these women do reach a facility after a long drive, they encounter a healthcare system with documented racial disparities in how patients are treated3,4. Distance is just the first barrier. It’s rarely the last.
For immigrant families, add language access and fear of navigating institutions that feel hostile. For single mothers, add the cost of childcare for older kids while getting to an appointment two counties over. The system wasn’t designed with any of these realities in mind. And that’s not an accident either.
What It Actually Costs
Women in maternity deserts are more likely to receive late or no prenatal care, not because they don’t want it, but because it isn’t there2.
Late prenatal care means undetected gestational diabetes. Unmanaged hypertension. Missed early warning signs for preeclampsia — conditions that are manageable when caught early and life-threatening when they aren’t.
The outcomes data is grim. Counties with no or low maternity access have higher rates of preterm birth and low birth weight, and poor access is linked to worse maternal outcomes overall1-4. The United States already has one of the highest maternal mortality rates among high-income nations, and women in maternity deserts carry a disproportionate share of that burden3,4.
Babies born in cars. Emergency deliveries in ERs that haven’t managed an obstetric case in years. These aren’t dramatic exceptions. They’re what happens when a system treats birth as optional infrastructure.
What’s Being Done — Slowly
There is movement on this, though not fast enough.
The Tech to Save Moms Act aims to expand telehealth access for prenatal and postpartum care, creating a meaningful lifeline when the nearest OB is an hour away5. Telehealth isn’t a substitute for hands-on obstetric care, but for routine monitoring and early warning detection, it closes real gaps.
Although the 2021–2022 Rural MOMS bills were not enacted by Congress, related rural maternal-health initiatives remain active through subsequent legislation and appropriations6. Similarly, pandemic-era telehealth flexibilities remain in force through a temporary extension, while Congress continues debating permanency.
The policy mechanisms exist. Whether they survive the current funding environment is a different question.
If You’re Pregnant and Living in a Desert
 This system needs to change. But while it’s changing, here’s what you can do right now:
This system needs to change. But while it’s changing, here’s what you can do right now:
Find your closest hospital with OB services before you need it. Not in month eight. Now. Know the route, know the drive time, have a plan.
Ask about telehealth. Many OB practices and Federally Qualified Health Centers offer virtual prenatal visits. It’s worth asking — and worth pushing for if it’s not offered7.
Connect with a community health worker (CHW) or doula8. In many underserved areas, CHWs can help navigate access, coordinate care, and be a consistent point of contact when the system feels impossible to reach.
Know your emergency warning signs. Severe headache, sudden swelling, vision changes, heavy bleeding, and reduced fetal movement can’t wait for an appointment. Get in the car.
Ask about transportation benefits. Medicaid covers non-emergency medical transportation in many situations, and other state or county programs may also offer ride support9.
You shouldn’t have to work this hard to have a safe birth. The fact that you do is a failure of the system, not yours.
The Bottom Line
No one should be in labor on a highway because the nearest delivery unit closed three years ago. That’s not a personal circumstance. That’s a policy outcome.
We built a world where “safe” depends on your zip code. We can build a better one.
References:
- March of Dimes, Nowhere to Go: Maternity Care Deserts Across the US. Report. Published 2024
- American College of Obstetricians and Gynecologists. Access to Care During Obstetric Emergencies. Issue Brief. Published 2025-06
- Verter F. We must keep working towards Birth Equity. Parent's Guide to Cord Blood Foundation Newsletter Published 2025-03
- Crear-Perry J. National Birth Equity Collaborative. New York State Task Force on Maternal Mortality and Disparate Racial Outcomes. slide show Published 2018-06
- Congress.gov S.958 - 119th Congress (2025-2026). Tech to Save Moms Act. Senate Bill Tracker. Accessed 2026-05-01
- Congress.gov S.1491/H.R.769 - 117th Congress (2021-2022)
The Rural Maternal and Obstetric Modernization of Services (Rural MOMS) Act. Senate Bill Tracker. & House Bill Tracker. Accessed 2026-05-01 - Dept. of Health & Human Services (HHS.gov). Telehealth policy updates. Last updated 2026-02-05
- Verter F. Health Insurance and Doulas. Parent's Guide to Cord Blood Foundation Newsletter Published 2025-03
- Centers for Medicare and Medicaid Services (CMS). RE: Assurance of Transportation: A Medicaid Transportation Coverage Guide. Published 2023-09-28