You are here




7 Myths & Realities about Perinatal Stem Cells
| Definitions of Perinatal Cells Umbilical Cord Blood (UCB) is blood from the blood vessels in the umbilical cord of a newborn that contains Hematopoietic Stem Cells (HSCs). Umbilical Cord Tissue (UCT) Surrounding the blood vessels in the umbilical cord is a tissue called Wharton’s Jelly that contains Mesenchymal Stem/Stromal Cells (MSCs). Hematopoietic Stem Cells (HSCs) are blood forming cells that can produce all types of blood cells, including white blood cells, red blood cells, platelets. Mesenchymal Stem/Stromal Cells (MSCs) are multipotent cells that produce cartilage, bone, fat. Native Cells refers to stem cells in their natural state within any tissue or organ. Ex Vivo Expanded Cells refers to cells have been isolated from their source tissue and “cultured” outside the body (ex vivo) in a laboratory to “expand” the number of cells.
| |||||||||||||||||||||||||||||||||
 | Myth #1: Only tissues from the time of birth, the “perinatal” tissues, have stem cells. Reality #1: Native stem cells naturally exist throughout the human body Perinatal blood and tissues are the richest source, but not the only source, of stem cells in the human body1,2. Example: HSC can be isolated from bone marrow, peripheral blood, and cord blood. The density of HSC is 1 per 100,000 bone marrow cells but 1 per 10,000 cord blood cells. Example: MSC can be isolated from multiple perinatal sources: umbilical cord blood, umbilical cord tissue (Wharton’s Jelly), amniotic fluid, amniotic membrane, placenta, and chorion. | |||||||||||||||||||||||||||||||||
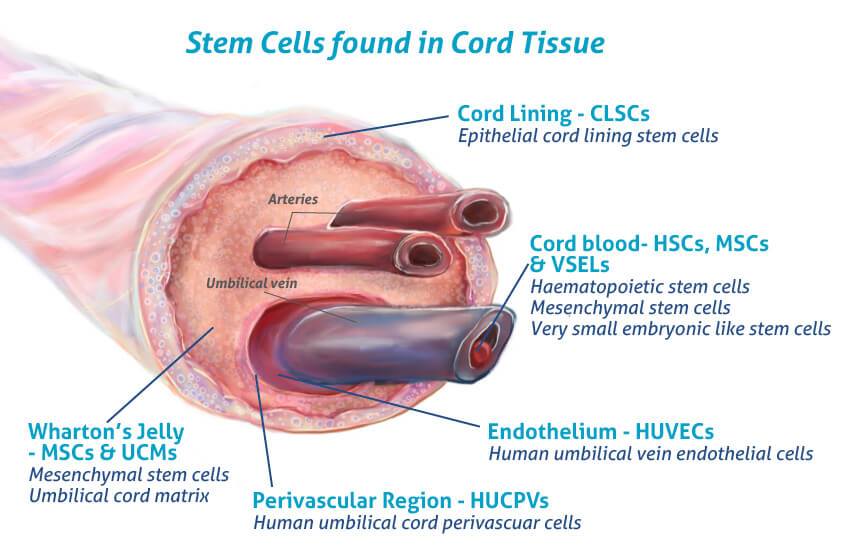 | Myth #2: The umbilical cord is full of stem cells. Reality #2: Both cord blood and cord tissue contain a mix of cell types, not just stem cells. Cord blood contains HSC, as well as red blood cells that carry oxygen, white blood cells that fight infections, and platelets that facilitate clotting3. Cord tissue contains more than one type of MSC, including MSC from the lining of the cord, the lining of the blood vessels, and the Wharton’s Jelly that fills the space around the blood vessels3,4. | |||||||||||||||||||||||||||||||||
.png) | Myth #3: Scientists figured out how to count numbers of stem cells years ago. Reality #3: To this day, there are no markers to exclusively identify stem cells. So far, laboratories have relied on measurements of surface proteins on cells in order to distinguish cell types. But these protein markers do not exclusively identify cell types. Therefore, all “measurements” of stem cell dose are always approximations2,5,6. Example: HSCs express CD34 and CD133, but not all CD34+ or CD133+ cells are HSCs! This is because CD34 & CD133 are also expressed after stem cells have partially evolved towards specific cell types, becoming what are called “committed progenitor cells”. Only about 1 in 100 cells that are CD34+ or CD133+ are actually HSC. Example: The accepted definition of MSC requires the following expression profile of cell surface protein markers: CD11b-, CD19-, CD29+, CD34-, CD44+, CD45-, CD73+, CD90+, CD105+, HLA-DR- | |||||||||||||||||||||||||||||||||
 | Myth #4: All methods of isolating MSC give the same result. Reality #4: Isolation method impacts the Quality and Quantity of MSC. This has been studied in detail for MSC isolated from the same umbilical cord tissue (UC-MSC), with or without using the enzyme collagenase to digest the umbilical cord and release cells. It is found that the cell surface protein markers of the MSC that were released by enzymes are different from native MSC that were not exposed to enzymes7. | |||||||||||||||||||||||||||||||||
| Myth #5: Expanding MSC simply increases their number but does not change their character. Reality #5: Native MSC and Ex Vivo Expanded MSC are NOT biologically equivalent. The expression of cell surface markers differs between Native MSC versus Ex Vivo Expanded MSC7. This is because the process of culturing the cells in the laboratory through growth cycles selects for MSC, enriching their concentration but also removing any companion cells that were part of the native environment. Hence, any difference in the manufacturing of MSC in the laboratory leads to a different MSC product. | |||||||||||||||||||||||||||||||||
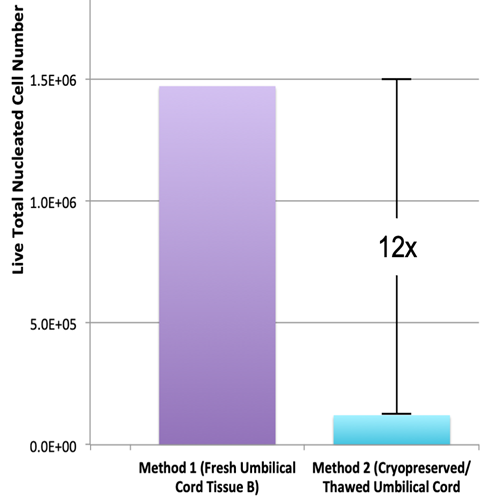 | Myth #6: Banking whole cord tissue is the same as banking MSC. Reality #6: Fewer viable MSC are retrieved from frozen tissue. When family cord blood banks offer their clients “storage of MSC from cord tissue”, almost all of them are freezing little chunks of tissue without extracting MSC. This has pros and cons. The major pro is that the process of getting regulatory approval for a therapeutic MSC product is deferred until the time that the cells are needed. The con side is that the ability to retrieve viable stem cells is always reduced after any type of blood or tissues have been frozen. Nonetheless, viable MSC can be retrieved from frozen umbilical cord tissue and Ex Vivo Expanded to sufficient numbers for therapy. There are debates in the literature about the character and efficacy of previously frozen MSC that are still under research8-13. | |||||||||||||||||||||||||||||||||
 | Myth #7: It doesn’t matter how much you expand MSC, they are still the same MSC. Reality #7: MSC gradually lose potency over multiple cycles of expansion. This is another example of how Ex Vivo Expanded MSC are not biologically equivalent to Native MSC. In terms of functional effect, animal models show that Ex Vivo Expanded MSC are weaker than Native MSC14,15. Hence, having greater numbers of MSC does not guarantee that they are all high quality MSC. In fact, the data suggest that ex vivo expansion results in accelerated senescence (aging) and exhaustion of MSC when they are cultured outside the body. When cells grow naturally in the human body, they are in an extremely complex environment which we cannot replicate in simplified laboratory cultures. | |||||||||||||||||||||||||||||||||
 | About the Author: Rouzbeh R. Taghizadeh, Ph.D. Dr. Rouzbeh R. Taghizadeh has dedicated more than 20 years to bringing stem cell-based therapies to clinical practice. His research has focused on the regenerative properties of human HSC and MSC, and how best to harness them for clinical applications. Dr. Taghizadeh co-founded AuxoCell Laboratories Inc. in 2008, where he worked as Chief Scientific Officer until 2023. At AuxoCell, Dr. Taghizadeh developed novel methods and technologies for the collection, processing, and banking of cell populations from the human umbilical cord for eventual utilization in cell-based therapies. Most notably, Dr. Taghizadeh and his team developed the patented AuxoCell Processing System (AC:Px®) in order to allow for standardized, efficient collection of cells (including stem cells), non-cellular matrix proteins, and morselized tissue from any number of human and non-human solid tissues in a closed, single-use, disposable system. Dr. Taghizadeh is the author of dozens of patents on cell and tissue processing techniques. Currently, Dr. Taghizadeh is working as a consultant, offering insights on cell therapy that fuse clinical utility with business savvy. Dr. Taghizadeh has presented at various scientific and industrial forums, he has contributed to numerous peer-reviewed publications and book chapters, and is an editor of multiple books focusing on Perinatal Stem Cells. |
.jpg)
References
- Lucie. Stem Cells Illustration. BIO-Grafik
- Zbinden A, Canté-Barrett K, Pike-Overzet K, Staal FJT. Stem Cell-Based Disease Models for Inborn Errors of Immunity. Cells 2022; 11(1):108.
- Taghizadeh RR, & Sherley JL. Expanding the therapeutic potential of umbilical cord blood hematopoietic stem cells. Perinatal Stem Cells 2009; Chapter 2, Pages 21-35.
- Cells4Life. Umbilical Cord Tissue Stem Cells – more valuable than you think. Blog published 2016-08-05
- Dutton R, Abdi F, Minnetyan L, Sherley JL. (2020) A Computational Simulation Technology for Specific Counting of Perinatal and Postnatal Human Tissue Stem Cells for Transplantation Medicine. OBM Transplantation 4(3):24.
- Sherley JL. Kinetic Stem Cell Counting. Parent’s Guide to Cord Blood Foundation News Published 2022-06
- Taghizadeh RR, Cetrulo KJ, Cetrulo CL. Collagenase Impacts the Quantity and Quality of Native Mesenchymal Stem/Stromal Cells Derived during Processing of Umbilical Cord Tissue. Cell Transplantation 2018; 27(1):181-193.
- Briddell R, et al. Blood 2011; 118(21):4398.
- Balci D & Can A. The assessment of cryopreservation conditions for human umbilical cord stroma-derived mesenchymal stem cells towards a potential use for stem cell banking. Curr. Stem Cell Res. Ther. 2013; 8(1):60-72.
- Moll, G. et al. Do cryopreserved mesenchymal stromal cells display impaired immunomodulatory and therapeutic properties? Stem Cells. 2014; 32:2430–42.
- Briddell R, Perinatal Stem Cells Isolated From Complete Umbilical Cord Tissue for Family Stem Cell Banking and Potential Therapeutic Use. Perinatal Stem Cells, Academic Press, 2018; Chapter 19, Pages 257-269.
- Skiles ML, Marzan AJ, Brown KS, Shamonki JM. Comparison of umbilical cord tissue-derived mesenchymal stromal cells isolated from cryopreserved material and extracted by explantation and digestion methods utilizing a split manufacturing model. Cytotherapy 2020; 22(10):581-591.
- Cottle, C. et al. Impact of Cryopreservation and Freeze-Thawing on Therapeutic Properties of Mesenchymal Stromal/Stem Cells and Other Common Cellular Therapeutics. Current Stem Cell Reports 2022; 8(2):72-92.
- Taghizadeh RR, Cetrulo KJ, Cetrulo CL. Wharton's Jelly stem cells: Future clinical applications. Placenta 2011; 32(S4):S311-S315.
- Galipeau J & Sensébé L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 2018; 22(6):824-833.