You are here




Red Blood Cells for Premature Babies as a product from Cord Blood Banks
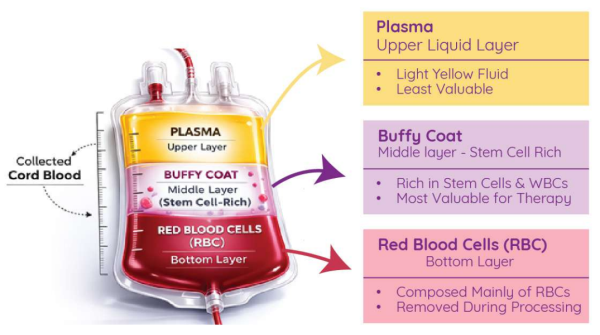
This is a story about turning trash into treasure. Traditionally, cord blood banks separate umbilical cord blood into three components: the blood plasma, the “buffy coat”, and the red blood cells (RBC). The buffy coat, which contains white blood cells and is rich in stem cells, is the part that cord blood banks cryopreserve. Most cord blood banks, both public banks and family banks, discard the plasma as well as the RBC.
Now, researchers have found that RBC from cord blood can play an important role in supporting premature babies. The clinical need for RBC from cord blood creates a market for a new product that can be supplied by cord blood banks. This gives rise to logistic questions: how should the operations of cord blood banks be modified to produce RBC products which meet the needs of these patients, and how can this be done in an efficient and cost-effective manner?
Medical need of Cord Blood RBC for Premature Babies
Extremely Low Gestational Age Neonates, those babies born before 28 weeks gestation and known as ELGANs, suffer from anemia of prematurity and often receive multiple small transfusions of RBC1,2. Traditionally, these transfusions have been supplied by blood banks that collect donations from adults.
But the RBC in newborn babies are not the same as the RBC in adult blood3. In the womb, babies produce fetal hemoglobin (HbF), which has a higher affinity for oxygen than adult hemoglobin (HbA). The fetal hemoglobin enables the fetus to pick up oxygen from the mother’s blood at the placental interface. After birth, the baby’s metabolism slowly turns off the production of HbF and switches over completely to producing HbA by the time the baby is a few months of age.
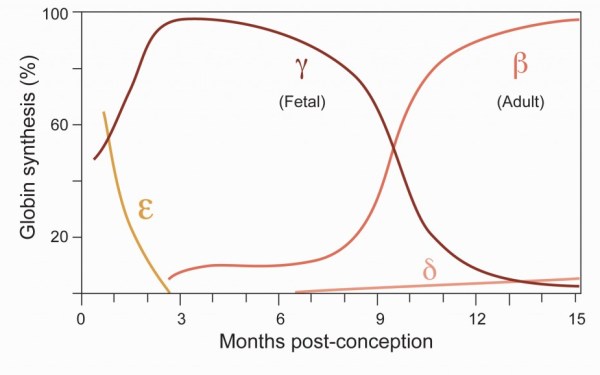
Image credit: Bauer Lab Functional Genomics of Hemoglobin Switching
In the case of ELGAN babies, they were born too soon and are still relying on fetal hemoglobin. When they receive repeated transfusions of adult RBC, it changes the composition of their blood from HbF to HbA. For many years, medical researchers have been concerned that replacing the blood of babies with adult blood was causing lower oxygenation of their organs. This could be a contributing factor towards multiple complications of prematurity, such as retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD), and necrotizing enterocolitis (NEC).
During the decade from 2000 to 2010, a number of researchers proposed saving the autologous cord blood of premature babies for use in perinatal transfusions, and a couple of studies tried this approach in Germany and the Netherlands4,5. The results were frustrating, because the most premature babies had the smallest cord blood collections and the highest transfusion needs. It became clear that ELGANs could not supply enough cord blood for their own transfusion needs. Efforts to transfuse very premature babies with cord blood would have to rely on allogeneic cord blood from donors. Starting in 2012, a group in Italy has run prospective clinical trials of this approach6-9.
Clinical evidence that RBC from cord blood benefits ELGANs
In a proof-of-concept clinical trial on 25 premature babies published in 2020, the group in Italy demonstrated that transfusions of RBC from cord blood preserve the level of fetal hemoglobin in the baby’s blood. “Every adult-RBCs transfusion increased the risk for an HbF in the lowest quartile by about 10-fold”8.
A phase 2 clinical trial of cord blood RBC versus adult RBC transfusions for ELGAN babies was conducted over the three years 2022 to 2024. The trial was named BORN, for “umBilical blOod to tRansform preterm Neonates”9. Across Italy, nine public cord blood banks and ten Neonatal Intensive Care Units (NICUs) participated in the BORN trial. The primary outcome measure was severe retinopathy of prematurity, which is a leading cause of blindness in children.
The BORN trial encountered some logistic difficulties but was nonetheless successful9. The study enrolled 142 ELGANs. The banks processed 451 cord blood units for RBC. The units were given to babies on the basis of ABO and Rh blood typing only. The 58 babies on the intervention arm of the study received 107 cord blood RBC transfusions and 111 adult RBC transfusions. Meanwhile, on the control arm 60 babies received 240 adult RBC transfusions. Notice that not all babies on the intervention arm received cord blood when they required RBC; this was where logistic difficulties interfered and we will discuss them below. Nonetheless, the group of babies that received cord blood RBC exclusively had significantly reduced incidence of severe retinopathy of prematurity (ROP).
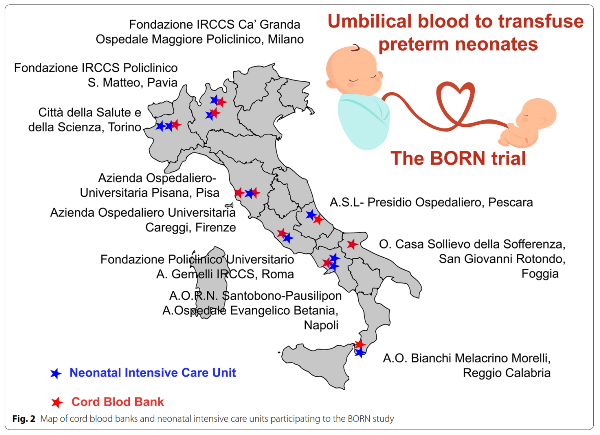
Image credit: Teofili L, et al. 2022; Trials. 23:1010. https://doi.org/10.1186/s13063-022-06949-8
Feasibility of Manufacturing RBC from Cord Blood
The primary logistical difficulty that arises when processing cord blood RBC for premature babies is that the RBC have a limited shelf life under standard blood-banking procedures. When the stem cells from cord blood are stored, they are cryopreserved at -196O Celsius and can be kept indefinitely. By comparison, RBC are normally stored at 4O Celsius for a few weeks. This creates a situation where the cord blood banks must continually produce more RBC units to replace expiring inventory. Gaps can arise where a baby needs a transfusion, but a fresh RBC unit is not available with the correct blood type. This is exactly what happened during the BORN trial, and is why the ELGANs on the intervention arm only received half of their transfusions from cord blood.
Two groups have conducted feasibility studies of the laboratory protocols for producing cord blood RBC to transfuse ELGANs. One is the Italian team behind the BORN study, and the other is a group in Spain10-12. The two groups follow similar protocols:
- Cord blood units were selected from donations to public banks that are too small for transplant (research units).
- Sterility cultures (bacterial and fungal) were started when the blood was collected.
- Instead of using standard cord blood processing procedures, a custom protocol was used to deplete leukocytes (white blood cells) from the cord blood. The two groups used different equipment.
- The separated cord blood RBC were stored at a temperature near 4O Celsius.
- The cord blood was irradiated with gamma rays prior to transfusion, or by day 14.
- Once irradiated, the cord blood RBC were transfused within 24 hours.
The time window during which a cord blood RBC unit can be transfused is bracketed on one end by the sterility cultures, which take 5-7 days, and on the other end by the irradiation step, which is performed by day 14. As a result, there is really only a one week window during which the RBC are available for transfusion.
Possible Improvements to Manufacturing RBC from Cord Blood?
1.Extending the storage time window
The biggest improvement to the existing protocol would be to extend the storage time window during which the cord blood RBC are available. One important question is whether the cord blood needs to be irradiated, and does this need to happen by day 14?
Blood components are routinely irradiated when they are given to a patient that is immune-compromised and might experience transfusion-associated graft versus host disease from residual T-cells in the blood product13. It is standard policy to irradiate blood components given to newborns, because they have underdeveloped immune systems14. However, that policy was adopted on the assumption that the donor is an adult, whereas cord blood is famous for triggering less graft versus host reaction than adult donors15. Nonetheless, because a transfusion reaction is almost invariably fatal, the safest course is to continue the preventative radiation.
It is not obvious that the cord blood RBC need to be irradiated by day 14. When adult RBC are stored for adult patients, they have a shelf life of 42 days with no irradiation16. When adult RBC are irradiated, their shelf life is shortened to 28 days13. In their feasibility study, the Spanish group found that cord blood RBC are much more vulnerable to radiation than adult RBC; they begin to develop significant hemolysis and elevated levels of potassium within 24 hours of irradiation12,17. But they also found that the 34 units of cord blood RBC in their study could be stored for 21 days and still fall within the acceptance criteria for hemolysis (see Supplement Table 1)12. More research is needed to accurately pin down the shelf life of cord blood RBC.
2.Manufacturing that integrates with standard operations
Another potential improvement to the existing protocol would be procedures that incorporate RBC retrieval into standard cord blood processing. This would enable banks to utilize the RBC they are removing from cord blood units going into storage, instead of allocating separate cord blood units for RBC production.
A very preliminary feasibility study of RBC retrieval during standard cord blood processing was conducted in June 2026 for this article. The study looked at RBC retrieval during Hespan processing at the laboratory of PBKM FamiCord in Warsaw, Poland. The upside was that 98% of the RBC were recovered, but the downside was that the residual leukocyte content was too high for clinical use. The level of residual white blood cells (WBC) in the RBC ranged from 24 - 115 x 106, whereas the current standards to prevent alloimmunization require this contamination to be less than 5 x 106 per unit18. Therefore, an additional leukocyte filtration step is needed to create an RBC product suitable for transfusion. A previous study by an international consortium of 12 public cord blood banks using BioNest equipment for processing found that post-processing leukocyte filtration is very effective at creating an RBC product suitable for neonatal transfusion19.
Size of the Need for Cord Blood RBC
Although ELGANs represent a tiny fraction of babies, they require a disproportionate share of healthcare resources. In the United States, extremely preterm (<28 weeks gestation) babies comprise 0.7% of live births20. Out of the 3.6 million US births in 2023, that amounts to over 25 thousand ELGANs. They are the most heavily transfused pediatric patients, receiving a median of 3 to 8 small transfusions per baby1,2. If it became standard practice to give transfusions of cord blood RBC to ELGANs in the US, it would require banks to produce over 100 thousand small cord blood RBC units per year. That is well beyond the recruitment capacity of US public cord blood banks, in fact it is close to the entire penetration of cord blood banking in a country where about 3% of babies have their cord blood privately banked or donated21.
The leaders of the BORN study in Italy call for cord blood banks to grow this therapeutic pathway by building partnerships with neonatologists and organizations that focus on premature babies. This “groundbreaking and sustainable therapeutic approach might be rapidly implemented in every blood bank, including low-income countries“22. The ability to implement transfusions of allogeneic cord blood RBC wherever NICUs are found will require regulatory approvals, which in turn will require harmonization of banking procedures to produce standardized RBC products.
As we have seen from the numbers for the US market, in many countries the existing networks of public cord blood banks are not banking enough cord blood to meet this demand. Then there are many countries which only have family cord blood banks but no public banks. Meanwhile, the existing cord blood banks, both public and family, are routinely separating RBC and discarding them. It is easy to imagine that with proper maternal consents and proper modifications of laboratory protocols, those RBC could be made available to premature babies, turning trash into treasure.
References
- Fabres J, Wehrli G, Marques MB, Phillips V, Dimmitt RA, Westfall AO, Schelonka RL. Estimating blood needs for very-low-birth-weight infants. Transfusion. 2006; 46(11):1915-1920.
- Puia-Dumitrescu M, Tanaka DT, Spears TG, Daniel CJ, Kumar KR, Athavale K, Juul SE, & Smith PB. Patterns of phlebotomy blood loss and transfusions in extremely low birth weight infants. J. Perinatology. 2019; 39:1670–1675.
- Kaufman DP, Khattar J, Lappin SL. Physiology, Fetal Hemoglobin. 2023; StatPearls. Treasure Island (FL): StatPearls Publishing.
- Eichler H, Schaible T, Richter E, Zieger W, Voller K, Leveringhaus A, Goldmann SF: Cord blood as a source of autologous RBCs for transfusion to preterm infants. Transfusion. 2000; 40:1111-1117.
- Khodabux CM, von Lindern JS, van Hilten JA, Scherjon S, Walther FJ, Brand A: A clinical study on the feasibility of autologous cord blood transfusion for anemia of prematurity. Transfusion. 2008; 48:1634-1643.
- Bianchi M, Teofili L,Giannantonio C, Landini A, Papacci P, Fioretti M, Romagnoli C, Zini G. Transfuse Neonates with Cord Blood-Derived Red Blood Cells: A Feasibility Study to Assess Allogeneic Cord Blood Unit Fractionation and Validation. Blood. 2012; 120(21):275.
- Bianchi M, Giannantonio C, Spartano S, Fioretti M, Landini A, Molisso A, Tesfagabir GM, Tornesello A, Barbagallo O, Valentini CG, Vento G, Zini G, Romagnoli C, Papacci P, Teofili L. Allogeneic Umbilical Cord Blood Red Cell Concentrates: An Innovative Blood Product for Transfusion Therapy of Preterm Infants. Neonatology. 2015; 107(2):81–86.
- Teofili L, Papacci P, Orlando N, Bianchi M, Molisso A, Purcaro V, Valentini CG, Giannantonio C, Serrao F, Chiusolo P, Nicolotti N, Pellegrino C, Carducci B, Vento G, De Stefano, V. Allogeneic cord blood transfusions prevent fetal haemoglobin depletion in preterm neonates. Results of the CB-TrIP study. Br. J. Haematology. 2020; 191:263-268.
- Teofili L, Papacci P, Dani C, Cresi F, Remaschi G, Pellegrino C, ... Vento G. Cord blood transfusions in extremely low gestational age neonates to reduce severe retinopathy of prematurity: results of a prespecified interim analysis of the randomized BORN trial. Italian J Pediatrics. 2024; 50:142.
- Pellegrino C, Papacci P, Dani C, Cresi F, Remaschi G, Ansaldi G, ... Teofili L. Cord blood red cell concentrates for preterm neonate transfusion: Insights from the multicenter BORN trial. Transfusion. 2026; Online Ahead of Print
- González EG, Casanova MA, Samarkanova D, Aldecoa-Bilbao V, Teresa-Palacio M, Busquets EF, Figueras-Aloy J, Salvia-Roigés MD, Querol S. Feasibility of umbilical cord blood as a source of red blood cell transfusion in preterm infants. Blood Transfusion. 2020; 19(6):510–517.
- Samarkanova D, Codinach M, Aran G, Guitart M, Valdivia E, Martorell LL, ... Querol S. Quality and stability studies of red blood cell concentrates from umbilical cord blood compared to their adult counterparts. Blood Transfusion. 2024; 23(2):147157.
- Thant M, Seheult JN. Irradiation. PathologyOutlines.com Last updated 2021-07-06
- Araiza-Atanacio I, Sáez-de-Ocariz M, Orozco-Covarrubias L. Transfusion-Associated Graft-Versus-Host Disease in Pediatric Patients: Clinical Features and Outcomes. Pediatric Dermatology, 2025; 42:267-272.
- Ponce DM, Politikos I, Alousi A, Carpenter PA, Milano F, MacMillan ML, Barker JN, Horwitz ME, American Society for Transplantation and Cellular Therapy Cord Blood Special Interest Group. Guidelines for the Prevention and Management of Graft-versus-Host Disease after Cord Blood Transplantation. Trans. Cellular Therapy. 2021; 27(7):540-544.
- Lee JS, Kim-Shapiro DB. Stored blood: how old is too old? J. Clinical Investigation. 2016; 127(1):100–102.
- Yoshida T, Prudent M, D’Alessandro A. Red blood cell storage lesion: causes and potential clinical consequences. Blood Transfusion. 2019; 17(1):27–52.
- Adane T, Enawgaw B. Human leukocyte antigen alloimmunization prevention mechanisms in blood transfusion. Asian J. Transfusion Science. 2023; 17(2):264-272.
- Samarkanova D, Codinach M, Montemurro T, Mykhailova L, Tancredi G, Gallerano P, ... Querol S; MultiCord12 Study Group. Multi-component cord blood banking: a proof-of-concept international exercise. Blood Transfusion. 2023; 21(6):526-537.
- Taylor GL, O’Shea TM. Extreme Prematurity: Risk and Resiliency. Curr. Probl. Pediatr. Adolesc. Health Care. 2022; 52(2):101132.
- Verter F. Percentage of births banking cord blood by country. Parent's Guide to Cord Blood Foundation. Newsletter Published 2020-01
- Teofili L, Papacci P, Orlando N, Bianchi M, Pasciuto T, Mozzetta I, ... Vento G. BORN study: a multicenter randomized trial investigating cord blood red blood cell transfusions to reduce the severity of retinopathy of prematurity in extremely low gestational age neonates. 2022; Trials. 23:1010.