Sie sind hier




Blaming Preeclampsia on the Placenta
What is preeclampsia?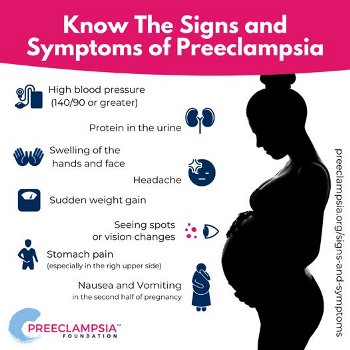
Eclampsia has been known since ancient times as one of the most serious complications of pregnancy. It is marked by the sudden onset of headaches and seizures, which can lead to coma, organ failure, and death. Eclampsia was first described by Hippocrates in the 5th century BC1. The name “eclampsia” (e-CLAMP-si-a) derives from the ancient Greek word for lightning, because eclampsia seemed to strike like a bolt out of the blue1.
Since the 1800’s, doctors have realized that eclampsia is preceded by preeclampsia, a period during which warning signs can be detected2. The key warnings of preeclampsia are elevated blood pressure (called gestational hypertension), as well as high levels of protein in the urine (called proteinuria)3. There are other symptoms that may be part of the pattern, such as decreased blood platelets, swollen ankles, or visual disturbances. Healthcare providers will look for the warning signs of preeclampsia at every pregnancy check-up.
How common is preeclampsia? 
Based on a review of over 11 million births in US hospitals, preeclampsia occurs in a little over 5% of pregnancies4. There are many studies which find that a mother’s ethnic and socioeconomic background influence her chances of being diagnosed and having a good outcome5,6.
Preeclampsia runs on the female side of some families, but roughly half of moms that are diagnosed with preeclampsia do not have a family history of the disorder7-9. A study of 1.4 million pregnancies in Denmark found that if you had preeclampsia in the last trimester of your first pregnancy, then you are ten times more likely to have it again with another pregnancy7. This factor of ten relative increase brings your total risk to about 20% chance of having preeclampsia again3,7. There are many factors that could change the risk for an individual mother, such as her age, her history of hypertension, how early in the pregnancy the preeclampsia started the first time, etc. A study of over a half a million women in Norway found that when preeclampsia recurs, the symptoms are less severe in subsequent pregnancies, so long as the pregnancies are less than a decade apart10.
How is preeclampsia prevented and treated today?
 There is a common myth that ending the pregnancy by delivering the baby will spontaneously “cure” preeclampsia within a couple of days. In fact, it can take weeks for preeclampsia to subside, so mom’s health should be carefully monitored during the postpartum period3. In rare cases, preeclampsia is first diagnosed during the postpartum period.
There is a common myth that ending the pregnancy by delivering the baby will spontaneously “cure” preeclampsia within a couple of days. In fact, it can take weeks for preeclampsia to subside, so mom’s health should be carefully monitored during the postpartum period3. In rare cases, preeclampsia is first diagnosed during the postpartum period.
To prevent preeclampsia when mom is at risk, doctors prescribe drugs to keep her blood pressure down. The first line of treatment is simply to take a daily baby aspirin11.
Preeclampsia can create a challenging medical situation if the mother is getting very sick and the baby is not yet full term. In this case, the mom will be admitted to the hospital so that she can receive a variety of treatments that are intended to both hold back the preeclampsia and at the same time prepare the baby in case of preterm birth. Mom will receive intravenous infusions of the drug magnesium sulfate to prevent seizures3,12. If mom has not yet reached 34 weeks gestation, she will also receive corticosteroids to accelerate fetal lung development13.
If you have been diagnosed with preeclampsia, you will need to rely on the expertise of your medical team. Preeclampsia is a notoriously complex condition, and the medical research is constantly evolving. For example, at one time obstetricians believed that giving magnesium sulfate not only prevented the mom from having seizures, but would also reduce the occurrence of cerebral palsy if the baby was born early14. Many pregnancy blogs claim that magnesium sulfate protects the baby’s brain, and as a result Google AI repeats this story12. But multiple careful studies have failed to prove that magnesium sulfate reduces cerebral palsy, and at the same time it has been found that too much magnesium sulfate carries other risks to the baby15-19. This is why a mom with preeclampsia should rely on guidance from medical professionals that have experience with this disorder, and are familiar with the latest research.
Why has preeclampsia been blamed on the placenta?
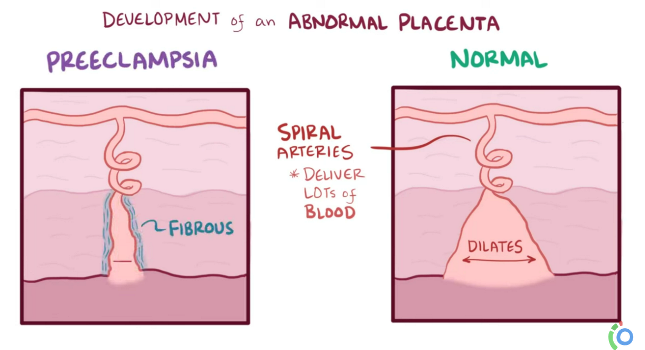
Over the past couple of decades, the prevailing opinion among researchers has been that preeclampsia is the fault of the placenta. It happens when the placenta does not attach deeply and properly to the uterine wall. As a result, the placenta suffers from low blood flow and inadequate oxygen supply. This stress causes the placenta to release signaling proteins that cross into the mother’s blood stream and damage the walls of her blood vessels, which causes high blood pressure, protein leakage into the urine, and systemic inflammation20-25.
The problem with blaming the placenta entirely for preeclampsia is that the placenta does not work alone. Where they touch each other on the uterine wall, the placenta and the mother’s metabolism are executing an intricate dance in which numerous signals are exchanged. It has long been known that not all cases of poor placenta attachment lead to preeclampsia, and not all women with preeclampsia have poor placental attachment21. A medical paper published in 2022, and cited over 300 times, asks if the placenta is “villain or victim”?24
The alternative explanation that is gaining acceptance is that the mother is at fault for preeclampsia. In women who have a predisposition towards cardiovascular issues, or a family history of preeclampsia, it is the maternal participation in the partnership that causes the placental attachment to the uterine wall to be weak24. Looking at the partnership between mother and placenta this way helps to explain the varied presentations of preeclampsia, and it makes it possible to set up screening programs so that mothers at risk can be identified earlier24,25.
Recovering from preeclampsia
 “It has been a long-standing belief that the harmful maternal consequences of preeclampsia are completely reversible with termination of pregnancy.”24 Unfortunately, we now know this is not completely true.
“It has been a long-standing belief that the harmful maternal consequences of preeclampsia are completely reversible with termination of pregnancy.”24 Unfortunately, we now know this is not completely true.
Mothers who have experienced preeclampsia during their pregnancy are at higher risk for cardiovascular problems later in life3,24,25,27. About 30% of women who had preeclampsia during pregnancy continue to have elevated blood pressure in the decade after childbirth24. “Not only does preeclampsia seem to predispose women to develop hypertension, but these women also develop hypertension at an earlier age, allowing the condition to add years to its impact on their bodies”25.
Children born from preeclampsia pregnancies also have somewhat higher blood pressure than their peers26,27. Researchers are still looking at the role of preeclampsia versus premature birth for this group of children.
The health risks for mothers and babies that went through preeclampsia should not be cause for alarm, but awareness of the long-terms impacts should motivate moms to be more vigilant about monitoring their blood pressure and maintaining habits that are good for their cardiovascular health.
References
- Wikipedia. Eclampsia. Accessed 2026-04-01
- Purkerson ML, Vekerdy L. A history of eclampsia, toxemia and the kidney in pregnancy. Am J. Nephrology. 1999; 19(2):313-9.
- Preeclampsia Foundation. FAQS. Accessed 2026-04-01
- Minhas AS, Ogunwole SM, Vaught AJ, Wu P, Mamas MA, Gulati M, et al. Racial disparities in cardiovascular complications with pregnancy-induced hypertension in the United States. Hypertension. 2021; 78(2):480-8.
- Yang Y, Le Ray I, Zhu J, et al. Preeclampsia Prevalence, Risk Factors, and Pregnancy Outcomes in Sweden and China. JAMA Network 2021; 4(5):e218401.
- Suresh S, Amegashie C, Patel E, Nieman KM, Rana S. Racial Disparities in Diagnosis, Management, and Outcomes in Preeclampsia. Preeclampsia. 2022; 24:87-93.
- Boyd HA, Tahir H, Wohlfahrt J, Melbye M. Associations of personal and family preeclampsia history with the risk of early-, intermediate- and late-onset preeclampsia. Amer. J. Epidemiology. 2013; 178(11):1611-9.
- Haram K, Mortensen JH, Nagy B. Genetic Aspects of Preeclampsia and the HELLP Syndrome. J. Pregnancy. 2014; 2014:910751.
- Gray KJ, Saxena R, Karumanchi SA. Genetic predisposition to preeclampsia is conferred by fetal DNA variants near FLT1, a gene involved in the regulation of angiogenesis. Amer. J. Obstetrics & Gynecology. 2017; 218(2):211-218
- Skjærven R, Wilcox AJ, Lie RT. The Interval between Pregnancies and the Risk of Preeclampsia. 2002; NEJM. 346:33-38.
- American College of Obstetricians & Gynecologists (ACOG). Low-Dose Aspirin Use During Pregnancy. ACOG Committee Opinion. 2018; No.743
- Bird C, RN, Dweck A. Reasons Why a Doctor May Prescribe Magnesium Sulfate During Pregnancy. Parents. Published 2024-04-16
- Roberts D, Brown J, Medley N, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database of Systematic Reviews. 2017; 3(3):CD004454.
- American College of Obstetricians & Gynecologists (ACOG). Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection. ACOG Committee Opinion. 2010; No.455
- Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, Iams JD, et al., for the Eunice Kennedy Shriver NICHD Maternal-Fetal Medicine Units Network. A Randomized, Controlled Trial of Magnesium Sulfate for the Prevention of Cerebral Palsy. NEJM. 2008; 359:895-905.
- Crowther CA, Ashwood P, Middleton PF, McPhee A, Tran T, Harding JE, for the MAGENTA Study Group. Prenatal Intravenous Magnesium at 30-34 Weeks’ Gestation and Neurodevelopmental Outcomes in Offspring. JAMA Network. 2023; 330(7):603-614.
- Shepherd ES, Goldsmith S, Doyle LW, Middleton P, Marret S, Rouse DJ, Pryde P, Wolf HT, Crowther CA. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database of Systematic Reviews. 2024; 5:CD004661.
- Grimes D, Nanda K. Magnesium Sulfate Tocolysis: Time to Quit. Obstetrics & Gynecology. 2006; 108(4):986-989.
- Elliott JP, Morrison JC, Bofill JA. Risks and Benefits of Magnesium Sulfate Tocolysis in Preterm Labor (PTL). AIMS Public Health. 2016; 3(2):348-356.
- Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005; 46(6):1243–1249.
- Singh HJ. Pre-Eclampsia: Is It All In The Placenta? Malays. J. Med. Sci. 2009; 16(1):7–15.
- Roberts JM, Bell MJ. If we know so much about preeclampsia, why haven’t we cured the disease? J. Reproductive Immunology. 2013; 99(1–2):1-9.
- Phipps EA, Thadhani R, Benzing T, Karumanchi A. Pre-eclampsia: pathogenesis, novel diagnostics and therapies. Nature Reviews Nephrology. 2019; 15:275–289.
- Melchiorre K, Giorgione V, Thilaganathan B. The placenta and preeclampsia: villain or victim? Amer. J. Obstetrics and Gynecology. 2022; 226(2S):S954-S962.
- Turbeville HR, Sasser JM. Preeclampsia beyond pregnancy: long-term consequences for mother and child. Amer. J. Physiology-Renal Physiology. 2020: 318(6):, F1315-F1326.
- Davis EF, Lazdam M, Lewandowski AJ, ... Leeson P. Cardiovascular Risk Factors in Children and Young Adults Born to Preeclamptic Pregnancies: A Systematic Review. Pediatrics. 2012; 129(6):e1552–e1561.
- Yang C, Baker PN, Granger JP, Davidge ST, Tong C. Long-Term Impacts of Preeclampsia on the Cardiovascular System of Mother and Offspring. Hypertension. 2023; 80(9):1821-1833.